CT physics for FRCR Part 1 explained
CT physics for FRCR Part 1 explained clearly, from attenuation and Hounsfield units to pitch, reconstruction, dose, and the most common artefacts tested.
Answer First
CT physics in FRCR Part 1 is mainly about understanding how attenuation becomes a reconstructed image, how image quality trades off against dose, and why common artefacts occur.
Key Facts
- FRCR CT questions are usually built around attenuation, Hounsfield units, reconstruction, pitch, slice thickness, and dose.
- The exam rewards relationships such as high pitch meaning faster acquisition with lower dose but less sampling.
- CTDIvol is a scanner output metric, while DLP adds scan length and should not be confused with patient-specific risk.
- Beam hardening, motion, and partial volume are high-yield artefacts because they connect physics to image appearance.
Practice
Apply this with real FRCR Part 1 questions
Reinforce today’s topic with targeted practice in the Spotters Academy app.
CT is one of the most important topics in FRCR Part 1 physics, but it is also one of the easiest to revise badly. Candidates often learn Hounsfield units, pitch, slice thickness, dose metrics, and artefacts as separate lists. That approach creates recognition without understanding. In the exam, that is usually where marks are lost.
The better way to study CT physics is to treat it as one connected system. X-rays pass through tissue, tissues attenuate the beam differently, detectors record those changes, the scanner reconstructs the data, and every parameter change alters the balance between image quality and dose.
What does FRCR Part 1 actually test in CT physics?
The exam is not trying to turn you into a CT engineer. It is testing whether you understand the principles that explain image appearance, image quality, and dose.
The recurring areas are:
- attenuation
- Hounsfield units
- windowing
- filtered back projection and iterative reconstruction
- slice thickness and spatial resolution
- pitch
- CTDIvol and DLP
- common artefacts
That is why CT links naturally to X-ray production and interactions and radiation dosimetry. The same concepts keep reappearing in a different form.
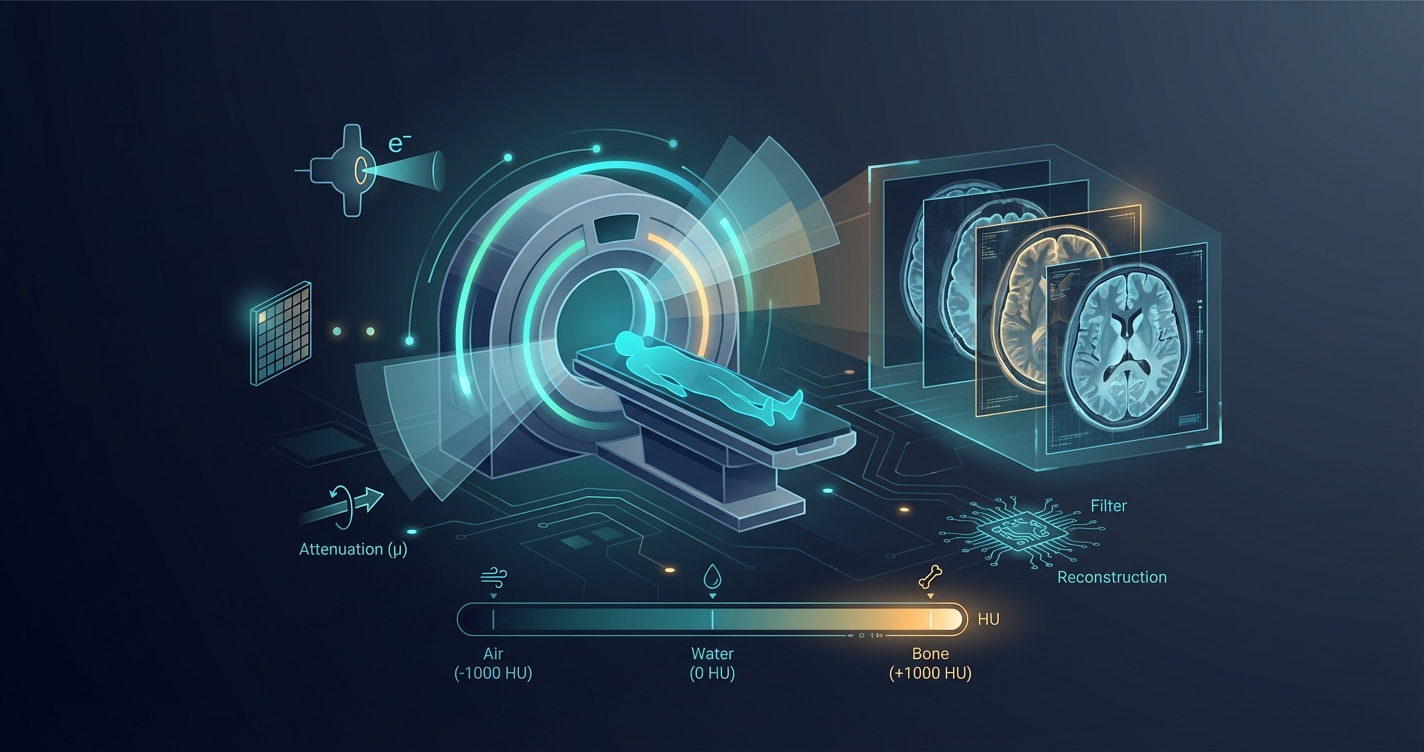
What is attenuation in CT physics?
Attenuation is the foundation of CT. If this part is clear, most of the rest becomes easier.
An X-ray beam passes through the patient and loses intensity as photons are absorbed or scattered. The degree of attenuation depends mainly on:
- tissue density
- effective atomic number
- photon energy
This is why air, fat, soft tissue, and bone are displayed differently. Air attenuates very little, so it appears black. Bone attenuates much more strongly, so it appears white. Soft tissue sits between those extremes.
In FRCR terms, the important point is not the wording of a definition. It is understanding that attenuation drives:
- CT contrast
- Hounsfield units
- beam hardening
- the trade-off between image quality and dose
How are CT images formed?
CT does not produce a direct photograph. It produces a reconstructed map of attenuation values.
The sequence is:
- The X-ray tube rotates around the patient.
- Detectors measure transmitted photons from many angles.
- The scanner converts those raw data into attenuation coefficients.
- Reconstruction algorithms generate the image you interpret.
That sentence about reconstruction matters. FRCR questions often test whether you understand that the image is mathematical, not optical. It explains why artefacts, interpolation, and reconstruction choices matter so much.
What are Hounsfield units?
Hounsfield units, or HU, express tissue attenuation relative to water.
The anchor points you need are:
| Tissue | Typical HU |
|---|---|
| Air | -1000 |
| Lung | around -500 to -800 |
| Fat | around -80 to -120 |
| Water | 0 |
| Soft tissue | around +20 to +60 |
| Acute blood | often +50 to +80 |
| Bone | commonly +700 and above |
You do not need a museum of exact values. You do need to know the order and the logic. A stem may ask whether fat attenuates less than water, or whether cortical bone sits above soft tissue on the HU scale. Those are easy marks if the relationships are clear.
Why does windowing matter in CT?
CT captures a very wide range of attenuation values, but the display screen cannot show every small difference at once in a useful way. That is why we use window width and window level.
- Window width changes contrast. A narrow width increases contrast between close values.
- Window level shifts the centre of displayed values and changes apparent brightness.
The exam point is simple: windowing does not change the data acquired by the scanner. It changes how those data are displayed for interpretation.
That is why a chest window and a bone window can show the same raw dataset in two very different ways.
What is the difference between slice thickness and pitch?
Candidates mix these up all the time.
Slice thickness
Slice thickness affects:
- z-axis resolution
- image noise
- partial volume averaging
Thin slices give better spatial detail but increase noise. Thick slices reduce noise but blur fine structures and increase partial volume effects.
Pitch
Pitch is usually described as:
table movement per rotation divided by total collimated beam width
In practical FRCR terms:
-
higher pitch means the table moves further per rotation
-
acquisition is faster
-
dose is usually lower
-
sampling is reduced, which can reduce image quality
-
lower pitch means more overlap
-
dose is usually higher
-
image data are denser
This is a favourite exam relationship because it joins speed, image quality, and dose in one variable.
What are the main reconstruction methods in CT?
For FRCR Part 1, you mainly need to compare filtered back projection and iterative reconstruction.
| Method | Main strength | Main limitation |
|---|---|---|
| Filtered back projection | Fast, historically standard | More image noise at lower dose |
| Iterative reconstruction | Reduces noise and can support dose reduction | More complex processing |
The high-yield statement is that iterative reconstruction can improve noise performance without simply increasing tube output. That makes it important in modern dose-optimisation questions.
You do not need advanced mathematics here. You need the practical consequence.
Which CT dose terms matter most in FRCR Part 1?
CT dose questions are common because they are clinically relevant and easy to ask badly-worded true or false questions about.
CTDIvol
CTDIvol is a standardised measure of scanner output within a reference phantom. It is reported in mGy.
What it is:
- a machine output metric
- useful for comparing protocols
What it is not:
- an exact patient-specific absorbed dose
- a direct measure of biological risk
DLP
DLP, or dose length product, is:
CTDIvol × scan length
It is reported in mGy.cm.
The key difference is that DLP incorporates the length of the examination. Two scans with the same CTDIvol can have different DLP values if scan length differs.
A quick comparison table
| Metric | Unit | What it reflects | Common mistake |
|---|---|---|---|
| CTDIvol | mGy | Scanner output in a standard phantom | Treating it as the patient’s exact dose |
| DLP | mGy.cm | Output adjusted for scan length | Treating it as equivalent to effective dose |
If you want the wider dose framework behind these terms, move next to radiation dosimetry for FRCR Part 1.
What are the common CT artefacts in FRCR Part 1?
Artefacts are high-yield because they test whether you understand the physics well enough to predict image appearance.
Beam hardening
Low-energy photons are absorbed more readily, so the beam becomes relatively higher energy as it passes through matter. This can produce:
- cupping artefact
- dark streaks between dense objects
Partial volume artefact
If one voxel contains more than one tissue type, the attenuation values are averaged. This can:
- blur small structures
- obscure sharp boundaries
- create misleading intermediate HU values
Motion artefact
Patient movement during acquisition creates:
- blurring
- streaking
- loss of detail
Metal artefact
Very dense material can produce severe streaking through photon starvation and beam-hardening effects.
The exam often asks what causes the artefact, not just what it looks like.
What are the most useful CT physics comparisons to remember?
| Parameter increases | Likely effect on image | Likely effect on dose |
|---|---|---|
| Slice thickness | Less noise, lower spatial detail | Often unchanged directly |
| Pitch | Faster scan, less sampling | Usually lower dose |
| Tube output | Less noise | Higher dose |
| Iterative reconstruction use | Less visible noise | Can permit dose reduction |
Tables like this are worth revising because they mirror how FRCR stems are built.
How should you study CT physics for FRCR Part 1?
Do not memorise the CT chapter as a list of isolated bullet points. Revise it in this order:
- attenuation
- Hounsfield units
- windowing
- slice thickness and pitch
- reconstruction
- dose metrics
- artefacts
That order works because each step supports the next one.
CT also sits naturally inside the wider FRCR Part 1 physics revision guide, where it should take more than one pass if physics is a weak area.
What mistakes cost marks in CT physics?
The usual problems are predictable:
- learning HU numbers without understanding attenuation
- confusing pitch with slice thickness
- saying CTDIvol is the patient dose
- forgetting that windowing changes display, not acquisition
- recognising artefact names without understanding their mechanism
These are not hard problems to fix. They just need deliberate revision instead of passive rereading.
Conclusion
CT physics is one of the highest-value topics in FRCR Part 1 because it compresses so much of imaging physics into one area. If you understand attenuation, Hounsfield units, pitch, reconstruction, dose metrics, and artefacts as one system, CT questions become much more predictable.
Use CT as a bridge topic. It connects cleanly to X-ray production and interactions, radiation dosimetry, and the wider FRCR physics study guide.
If you want to test whether these concepts are truly secure, use timed practice rather than more notes. Spotters Academy gives you 100 free credits to start.
Sources and further reading
Checked on 10 June 2026 for exam-format and radiation-guidance references.
Sources
Dr. Gayathri Priyadharshinee
Expert content from the Spotters Academy team. We're dedicated to helping radiologists succeed in their FRCR Part 1 examination.
Ready to ace your FRCR Part 1?
Join thousands of successful candidates who prepared with Spotters Academy.
Start Free Trial